|
 Search Site
Search Site |
|
Latest Additions |
|
News |
|
Mailing List |
|
Topic Index / FAQs |
Declassified
Documents |
|
Medical Information |
|
Navigation |
|
Organization |
|
Library |
| Related
Sites |
|
-
|

|
- CURRENT NEWS
|
|
- CASE NARRATIVES
|
|
- ENVIRONMENTAL EXPOSURE REPORTS
|
|
- HELP FOR VETERANS
|
|
- E-MAIL
|
-
|
-
|

|
- Leishmaniasis
- Cutaneous, Visceral, Mucocutaneous
-
- In 1988 this is a word that even tourist
barely heard from
- the State Department as a travel
warning. A little known third
- world disease that was quite
misunderstood. All the way back
- to its Scottish origin of Sir William
Boog Leishman in 1903.
-
- Physicians Leishman, and Donovan
discovered the cause
- of a tropical disease known as Kala-Azar,
caused by a
- parasite spread by sandfly bites. It was
a stained slide that
- showed Leishmania donovani for
the first time.
-
- Even though Leishmania tropica
and other variants had
- been seen before 1903, it wasn't really
understood until
- the public explanation by Leishman and
Donovan.
-
- Leishmaniasis is commonly seen in
tropical / sub-tropical
- regions of Africa, Mediterranean,
Southern Europe, Asia,
- and South & Central America. Its
estimated that 12 million
- people are currently infected. 367
million are at risk of getting
- leishmaniasis in 88 countries.
-
- During the first Gulf War, it was
claimed that only 20 cases
- of L. Major ( Cutaneous
Leishmaniasis ) surfaced among the
- soldiers coming back. That 12 cases of L.
Tropica ( Visceral
- Leishmaniasis ) were diagnosed up to
1993.
-
- To understand the strains and types,
there are a few technical
- notes that have to be spelled out. The
disease has two parts in
- its lifespan, the Zoonosis and the
Anthroponotic. The
- Promastigotes with tails starts in the
Sandflies, and the
- small internal round amastogote version
thrives in human's.
-
- The three different strains listed as
Cutaneous, Visceral, and
- Mucocutaneous exhibit different
symptoms. Cutaneous is
- skin, Visceral in internal organs, and
Mucutaneous as related
- to nasal or other mucous regions of the
body.
-
- At the point of contact of the sandfly
in Cutaneous Leishmaniasis,
- the Sandflies saliva is ejected onto the
bite - in that saliva the
- L. Tropica promastigotes
burrow into the wound. From there
- they swarm in the wound until the
ulceration becomes visible.
- Which becomes a long festering wound
that doesn't seem to
- heal for several months. This type of
external wound will heal
- in a year or so, but its uncertain if
the person ever is completely
- free of the organism. Scarring is a
factor, and wounds by eyes
- or other sensitive areas is a serious
concern. The disease can
- also lay dormant for many years before
recurring in a later cut
- or infection. But most of the time it
resolves in a non-threatening
- manner. The persons immune system is
able to suppress it.
-
- Visceral Leishmaniasis is much less
understood, and a much
- darker version of this parasite. Its
transmitted also by the same
- Sandflies, and in the bite wounds like
Cutaneous. After that its
- different in its lifecycle. It burrows
deep into the organs, bone,
- of the host. The early stages of the
disease are so subtle
- that a person might not know for several
years they have it. It
- so small that it doesn't show up in
normal blood test, or even
- in early tissue biopsies. Then when the
disease is in it latter
- stage does it start to make itself
known. Once the Spleen
- becomes enlarged, and the belly extends
does it start making
- it presence noticed. The strains of
Leishmaniasis are usually
- noted to be L. Infantum ( Infant
Syndrome ) or L. Donovani.
-
- Incubation period is considered between
3 to 33 weeks.
- That diagnosis being made largely though
a bone marrow
- biopsy, and or splenic asparate. (
tissue sample from bone
- marrow or spleen ). PCR ( DNA enzyme )
testing is still
- considered unreliable in confirming this
disease in 2005.
- The newest test being a dry PCR to the
wet PCR. Today
- its largely found as a stained gel slide
where someone
- sees the amastogote in a cell, same as
1903.
-
- What does a L. Donovani
amastogote usually look like, a
- cell with several nucleus parts to
it. The closest rough
- description would be a clear sack
with multiple nucleus
- spheres in it instead of one. A
clear marble with a clover
- like center. Without the
features of a expected parasite,
- its often overlooked - and even
missed by laboratories
- looking for it specifically. Its when
the parasite is in its
- late stage at 10 to the 15th power
number of parasites,
- and swarming that researchers are able
to diagnose it.
-
- The only American institution dealing
with this disease on a
- regular basis is Walter Reed Army
Hospital in Washington,
- DC. They work in conjunction with the
Armed Forces Institute
- of Pathology to track, type, and treat
this disease in troops
- coming back from Afghanistan and or
Iraq.
-
- Suspected number of current cases of
Cutaneous Leishmaniasis
- in these regions in American troops from
January 2003 to May
- 2005 has been 848. Visceral has been 4
cases of L. Infantum
- in that same period.
-
- However, more than 200,000 citizens of
Kabul Afghanistan were
- diagnosed with Cutaneous Leishmaniasis
in 2003 by the World
- Health Organization. So chance of
contagion there is high.
-
- In December 2003 the FDA held a blood
banking seminar to
- discuss the possibility of contamination
of the nations blood
- supply by Leishmaniasis. It was there
that the FDA decided a
- lifetime ban on blood donations from
persons diagnosed with
- Leishmaniasis from Iraq should be
imposed. Later the Pentagon
- would make the same policy of us troops.
Why a lifetime ban?
-
- Because at this time there is no
guarantee of a 100% sterile
- cure of any version of Leishmaniasis.
That fact was eluded to
- by Barbara Herwaldt of the CDC when she
presented her Power
- Point to the VA Advisory Committees on
Gulf War Veterans
- that I served on in 2008-2009. ACGWV
CDC 2009 presentation
-
- By 2004 more than 1,500 soldiers�contracted Leishmaniasis in
Iraq that was not reported correctly.� First they said 253, then 500,
then 600, then 1,000 and the story�changed much of 2004. At this
time the screening method was�mostly visual based on skin
lesions. Very few had blood samples�sent to Walter Reed for
examination.
-
- At the May 2005 Institute of Medicine
Infectious Disease
- meeting, Dr. Alan Magill of Walter Reed
Army Hospital had
- pointed out to the committee the
dark sides of Leishmaniasis.
- Part of which has been outlined in
this over view.
The average American has never heard of this disease and general
medicine is not prepared to deal with foreign diseases. So as
these people developed symptoms that had no recourse. I heard
from one person who approached Walter Reed for blood testing
only to find them disinterested in identifying it. You need a genome
type of the strain to identify which species as there are several
in Iraq. L. Tropica and L. Major are the dominate ones. Oddly enough
we introduced L. Mexicana from troops that brought it to Iraq. It
seems Walter Reed doesnt want to know the exact strains, maybe
because identifying its point of origin would make the Pentagon
responsible for its spread. -
- Here is a snippet of a 2006 WRAMC
publication:
-
- Transfusion.
- 2006 Sep;46(9):1641-5.
- Leishmania: risk to the blood supply.
Cardo LJ1.
Author information
� 1Walter Reed Army Institute of Research, Silver Spring, Maryland 20910, USA.
Lisa.Cardo@us.army.mil
- Operation Iraqi Freedom and Operation Enduring Freedom
present a much greater Leishmania threat than did Operation
Desert Storm. Because most transmission by transfusion
occurs in endemic areas, and visceral infection is asymptomatic
in healthy individuals such as blood donors, it is difficult to
determine the absolute risk of transmission by transfusion, but
review of the literature provides many clues as to the appropriate
measures to be taken for blood donor deferral.
- We at DSBR believe there are many more
cases of Leishmaniasis
- undiagnosed in America. That American
contractors serving
- in Iraq are coming home with it,
soldiers, tourist. That the
- diagnostic system in place across
America are missing this
- outbreak, and that in time it will be
spread here through
- transfusion, intimate contact, and
possibly mosquito vectors.
- Further, between troops from Iraq and
Afghanistan that served
- upwards of 5 tours - how many of those
might have been infected
- with any form of this parasite that was
never seen by any medic
- or reported. Could it be for every case
there was one that didnt
- report? 3, 5 or more. These people are
donating blood any time
- they want the rest of there lives.
Meaning every time is like adding
- another person to mix. Thousands of
possible tainted blood
- samples randomly mixed with health and
no screening system
- in place to detect this.
-
- Once infected the medical system wont
point back to tainted
- blood but imply some other vector.
Leishmaniasis positive people
- in America are treated the same as third
world individuals, and
- have no rights under the current system.
Once you have it, they
- dont care how you got it. You pay out of
your own pocket to
- treat it, live with it, and even be
mocked you claim to have it. This
- is a orphan disease and why its ignored
in America.
-
- The Pentagon simply is hoping it will
resolve itself when the
- small number of infected people in
America die off. Exceptable
- loses versus owning up to the
infiltration. But, there is no public
- tracking system or effort to follow this
so the number spreading
- are uncertain for up to 40 years.
-
- Testing can be done for the military at
Walter Reed Army
- Hospital, through Peter Weina at
301.319.9956 or email
- peter.weina@na.amedd.army.mil
http://www.pdhealth.mil/downloads/Leishmaniasis_DS_04272004.pdf
-
- There is also the Armed Forces Institute
of Pathology,
- which has a Leishmaniasis Registry.
Point of Contact
- is Colonel Peter McEvoy mcevoy@afip.osd.mil
- http://www.afip.org/leishsurvey.html
-
- If you are a civilian contractor, you
can go through
- Parasitic Disease Consultants
- http://parasiticdiseaseconsultants.com
- A Clinical Laboratory for the Diagnosis
of Parasitic,
- Viral and Other Infectious
Diseases.
- IRVING G. KAGAN, Ph.D, Director
- Mailing Address:
P.O. Box 616
Tucker, GA 30085
Laboratory Address:
2177-J Flintstone Drive
Tucker, GA 30084
- Phone # (770) 496-1370 / (770)
496-5848
Fax # (770) 938-7189
- The CDC has a Leishmaniasis testing
department, which you
- will go through Mr. Frank Steurer at
770-488-4475. http://www.cdc.gov/ncidod/dpd/parasites/leishmania/factsht_leishmania.htm
-
- This is the VA protocol for
dealing with Leishmanisis:
- http://www1.va.gov/environagents/docs/USHInfoLetterIL10-2004-013.pdf
-
- At the IOM May 2005, Dr. Alan Magill
said he did not know a
- Arvid Brown of Michigan. Here is a
copy of the July 12th 1998
- WRAMC letter to VAMC Ann Arbor
Michigan of the first ELISA
- test results on Arvid Brown. From the
book:
- "Bloodmeal:
ignored to death"
-
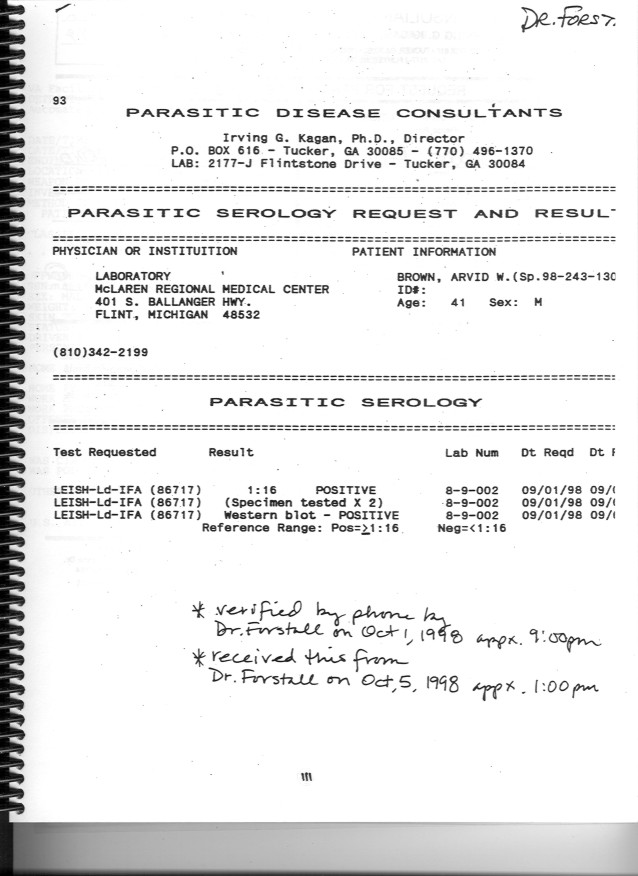
- The independent lab "Parasitic
Disease Consultants"
- confirmation of Arvid Browns
Leishmaniasis in 1998
- "Bloodmeal:
ignored to death" page 2
-
- IOM:
- Gulf War and Health: Infectious
Diseases
Project Identification Number: HPDP-H-04-06-A
http://www.gulflink.org/iom4/iom4.htm
- Slides of Richard Reithinger, Craig
Hyams,
- Mike Kilpatrick, Alan Magill
-
- CDC:
- Barbara Herwaldt slides to
- December 2003 FDA Blood bank committee
- CDC
Leishmaniasis Slides
-
- Kirt Love slides to the
- December 2003 FDA Blood bank committee
- Kirt
Love Leishmaniasis Slides
-
- Letters to DHSD from DSBR before the
was
- in Iraq of March 2003
-
- August 3rd, 2002
- Response
to Kirt Love on Leishmaniasis - page 1
- Response
to Kirt Love on Leishmaniasis - page 2
-
- September 20th, 2002
- Janyce
Brown to DHSD, 3 pages
-
- November 15th, 2002
- response letter from DHSD
- DHSD
response letter
- May 2003
- response from DHSD
- Response
to Kirt Love May 2003 page 1
- Response
to Kirt Love May 2003 page 2
-
- Freedom Magazine
- Volume 35 issue 1
- Desert
Storm Blows Back with a Fury
-
- Deployment Quarterly Spring 2005
- Quick Testing
Approved For Leishmania Parasite
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}